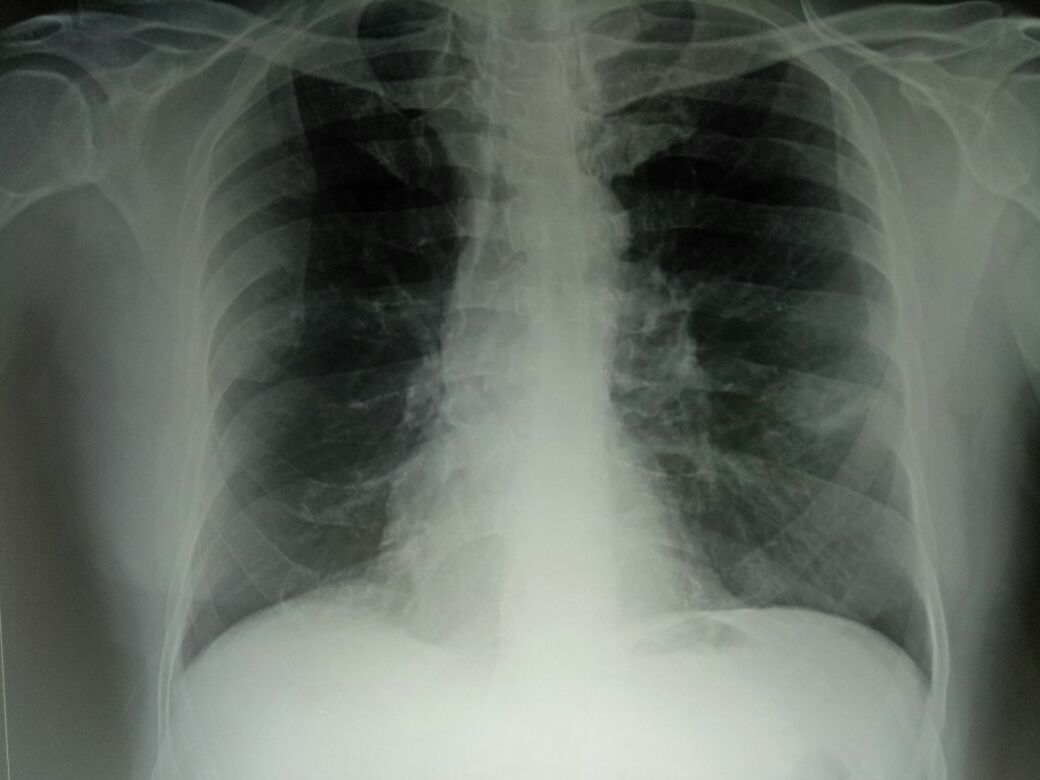
This is a 55 year old man in ICU with severe hypercapnia refractory to positive pressure ventilation with PCO2 ranging from 100-120 mm of Hg after 24 hours of ventilation. He appeared to have a history of Bronchial asthma since childhood. Perhaps for the last 45 years. His last three years appear to have been spent in perennial shortness of breath and wheeze. He has a barrel shaped chest and his CXR pa shows pushed down diaphragms. He was referred from a nursing home on a ventilator ambulance and his ABG during admission was showing a PCO2 of 90. After 24 hours of ACMV with a RR of 20 and tidal volumes of 400 ml his PCO2 increased to 120s.
This case of AECOPD with resp. Acidosis on mechanical ventilator was found to have total WBC count increasing overtime (15300 (ICU 2nd Day)/ 18500/ 27500/ 35600 (13th day). So, we started empirically with Clavum & Augmentin and later on planned for meropenam & Colistin antibiotic based on further deterioration in Total WBC Count.
Then CXR followed CT scan of lung was done which showed patient is having right upper lobe pneumonia. Then we had a dilemma between "Sheath vs non-shealth bronchoscopy". After searching on literature we found that shealth bronchoscopy is most preferred as chances of contamination is less but we also found that ET Tube suctioning is as good as sheath bronchoscopy. Hence, we went for ET suctioning for C/S. And report came on 14th day which had shown "Heavy growth for Actinobactoer species & Pseudomonas Aeruginosa" which was sensitive only to Polymyxin- B & Colistin. After that meropenam was discontinued and colistin was left continued on 14th day.
Patient was improving and shifted to SICU. But the patient developed hypokalemia & metabolic alkalosis and then patient was infused with KCL and today it was found that patients Total wbc count dropped to 15000 and patient is feeling much better and patients Hypokalemia and metabolic alkalosis also improved.
Old CT Scan Films:
































Patient got admitted again in Kolkata because of emergency and diagnosed with pneumonia, then got tumor in CT scan, then dr. tried FNAC but couldn't do successfully because it was shrimp like. then dr. adviced FOB and pneumonia relieved and WBC count from 30000, came to 8000 and person got discharged on own risk because didn't wanted to continue staying admitted.
He wants to know doses of medicine as doctor in the hospital told to take foracort rotacap 4 times/day and ipraventonce daily. Apart from this they advised to stop tenzact injection antibiotic and to take only sirf M-cin tablet once. Apart from this what will be the best option for me to get his FOB or FNAC done and do he needs to get admit again for this sort of test?




He is currently in KIMs hospital for his FNAC but repeat CxR pa and Usg chest shows no mass.
This comment has been removed by the author.
ReplyDeleteWe conclude that PTC is at least as accurate as PSB in the bacteriologic diagnosis of nosocomial pneumonia in intubated patients, and that its use can result in substantial cost savings, especially when fiberoptic bronchoscopy is not otherwise indicated. https://www.ncbi.nlm.nih.gov/pubmed?term=2024814
ReplyDeleteThe results of this study are consistent with the notion that blind PSB sampling and quantitative culture may prove to be a useful, cost-effective, and minimally invasive method of diagnosing VAP.
https://www.ncbi.nlm.nih.gov/pubmed?term=7606959
It is more sensitive and noninvasive, BBS is preferable to PSB for the diagnosis of VAP.
https://www.ncbi.nlm.nih.gov/pubmed?term=8520766
Using semiquantitative bacteriologic analysis, the sensitivity and the specificity of the protected mini-BAL in the diagnosis of nosocomial BPN were found to be 70 and 69%, respectively. Protected mini-BAL identified 77% of causative microorganisms of BPN.
https://www.ncbi.nlm.nih.gov/pubmed?term=1416397
Minibronchoalveolar lavage is a safe and technically simple procedure for obtaining quantitative lower airway cultures in patients requiring mechanical ventilation. Quantitative culture results obtained by minibronchoalveolar lavage are similar to those obtained by the protected specimen brush technique.
https://www.ncbi.nlm.nih.gov/pubmed?term=7717596
The operating characteristics of the EA technique (when taking the 10(6) cfu/ml of respiratory secretions as the interpretative cutoff point) compared favorably with those of the PSB technique. Diagnostic accuracy rates were similar. The specificity of EA was somewhat lower (83 versus 96%), but the sensitivity was higher (82 versus 64%).
https://www.ncbi.nlm.nih.gov/pubmed?term=8317789
Specimens obtained via bronchoscopy — Bronchoscopy can be used to acquire samples of lower respiratory tract secretions in patients with suspected pneumonia in whom respiratory samples cannot be obtained by expectoration or in whom such samples have been nondiagnostic. Lower respiratory specimens can be obtained by bronchoalveolar lavage, routine brushing, washing, or protected specimen brushing (using a double-sheathed catheter that minimizes bacterial contamination). A variety of quantitative culture methods have been developed to differentiate infection from colonization and to identify pathogenic organisms in the fluid obtained, but none of these methods is completely reliable. The utility of quantitative cultures of specimens obtained by bronchoscopy has been highly variable in individual patients and in various studies. The role of bronchoscopic sampling and quantitative cultures, which have been best studied in patients with ventilator-associated pneumonia, are discussed separately. (See "Clinical presentation and diagnosis of ventilator-associated pneumonia", section on 'Respiratory sampling'.)
When bronchoscopy is used, it is imperative that specimen handling be optimized, since fastidious organisms may not survive prolonged transport times. In addition, use of a diluent such as bacteriostatic saline in bronchoalveolar lavage or brush specimens can inhibit the growth of microorganisms, possibly leading to false-negative results [8].
Bronchoscopy for specimen collection is most useful for the diagnosis of infection due to Mycobacterium tuberculosis in patients with negative sputum studies, for P. jirovecii (formerly P. carinii) or other fungal or viral pathogens, or for establishing a noninfectious etiology such as malignancy.
Thanks Vivek, Here's something introductory from my searching: " For microbiologic propose the protected specimen brush (PSB) is contained in a protective sheath and covered by a biodegradable plug, thus avoiding contamination during passage through www.sciencedirect.com/science/article/pii/S0873215912000074 working channel"
ReplyDeleteThanks Vivek please share more about the value of psb from uptodate.Meanwhile read this https://ccforum.biomedcentral.com/articles/10.1186/cc431 and provide your inputs
Comment after sharing Vivek's evidence above by RB: So although it doesn't answer our original question of sheathed (protected) Vs unprotected as no one may have logically justified such a trial but we now know that what we have already done in this patient I e protected but blind ET tube sampling is perhaps good enough and an unprotected bronchoscopy sampling may not help. Ask Sanchali to add these to her icmr project qualitative learning points
Doctors prescribe Foracort for treating symptoms of COPD and asthma. Foracort inhaler makes breathing easier by relaxing the muscles of the airways. It is a combination inhaler for treating moderate to severe COPD (Chronic Obstructive Pulmonary Disease). It comes in different strengths and packaging, pick the one as per your requirements.
ReplyDeleteSeroflo 125 Autohaleris used to assist with asthma and chronic obstructive aspiratory disease in individuals who need normal therapy. Asthma is a condition affecting the lungs. Seroflo medication is Extremely effective in improving the manifestations of breathing challenges because of asthma.
ReplyDelete