UPDATES FROM HER HOSPITAL ADMISSION DURING THE WINTER OF 2018
Patient history before hospitalization:

Presentation notes containing the post hospital intervention part of her history:















Her past full medical records:
http://www.udhc.co.in/INPUT/displayIssueGraphically.jsp?topic_id=1780
http://globaludhc07.blogspot.in/2016/01/a-40-years-old-woman-with-nasal-tumar.html?m=1

Conversational discussion in Tabula Rasa:
Histopathology slides of 40 yrs female with nasal growth.
Slides:






Dr. Rakesh: Thanks for sharing these DrIshan. You and your team have reported it as Hemagiopericytoma and her previous biopsy from People's 3 years back was Hemangioma. Her complete record and previous discussion in tabula rasa can be found here:http://www.udhc.co.in/INPUT/displayIssueGraphically.jsp?topic_id=1780
Dr. Rakesh: Currently our surgeon needed to know from the group if we should go for pre-op radiotherapy to shrink the tumor or go ahead with the surgery and radiate her later. (Inputs Dr Prakash, Dr Chandra, Dr Swapnendu, Dr Mahendra Kr Jain ). Dr Mridul, Dr Nitin, Dr Paritosh, Dr Swagata, would be good to have your advice for our surgeon on how to avoid potential neuro-surgical complications after going through the CT scans available in the record above (and a sample here:http://www.udhc.co.in/ViewImage?file_id=9497&scale=800) Prof Upreet your inputs on the potential ophthalmic risks?
Dr. Rakesh: Bhavuk would be great if you can share your plan for this patient here.
Dr. Rakesh: Thanks Prof Upreet, Surprisingly her vision in both eyes is perfectly intact and there appears to be a displacement of the globe only without any nerve compression (no diplopia either). We are examining her fundus today and will keep you updated. The most important thing we need to decide today is pre-operative vs post operative radiotherapy. The postulated advantage of pre-op radiotherapy would be to shrink the tumor with its attendant vascularity (see this other CT image here:http://www.udhc.co.in/ViewImage?file_id=9506&scale=800) and make it easier to remove. The postulated disadvantage is that it may not work. We need to know if/when this or other approaches may have worked. Even a literature search would be of immense help (Priyank, Vasumathi, Bhavik, Pranab, Amy, Able, Ashwin, Prof SP Kalantri). Pratyush Ranjan for inputs
Dr. Vasumathi: Will look at this later in the day. About to take a flight back home
Dr. Swagata: I think preoperative RT will be a better option
Dr. Bhavuk: Good morning sir, sorry for late reply. Well surgical plan by far is, either a bicoronal approach, to enucleate the tumor from superior approach, or bilateral eyebrow approach, to access the pathology anteriorly, removal of entire tumor in toto, followed by comprehensive reconstruction by a temporalis myofacial sling to create inferior support for the globe and probably free bone graft secured with plates and screws for nasal bridge formation. Maxillary sinus will be approached intra orally to completely remove the tumor, which has already extended into Antrym of Hygmore. Reconstruction of maxilla by illiac crest corticocancellus graft.
Dr. Bhavik Shah: "The local control, disease-free survival, and overall survival rates appear to be greater when patients receive RT [109-111], but the efficacy of adjuvant radiation remains under study.
The natural history of hemangiopericytomas is illustrated by a series of 39 cases resected over a 24-year period at one institution [111]. The mean follow-up was 10 years. The actuarial recurrence rates at 1, 5, and 15 years were 4, 46, and 92 percent, respectively. Extraneural metastases occurred in eight patients (26 percent of those with follow-up data), at an average of 10 years after the original resection. The mean overall survival for the group was 18 years, and 13 patients died from their tumor during follow-up. There appeared to be an improved recurrence-free survival in those who were able to undergo a complete resection and then received adjuvant external beam radiation therapy.
In selected cases of recurrent disease following RT, chemotherapy may be helpful [112]. Novel treatments including anti-angiogenic therapies are being evaluated for extracranial hemangiopericytomas [113] and could also have a role for intracranial disease"
Courtesy - UpToDate
I've not gone through the patient's history, but it seems that total removal f/b adjuvant chemo and/or radiation seems a better option.
Maybe drugs like Bevacizumab can also be useful post removal (in case, patient can afford it).
But have to go though the literature!
Dr. Bhavuk: Bhavik Shah thanx for the emaculate evidence based comment. I second your opinion, pre op RT might shrink the lesion but could possibly lead us to insufficient excision, what do u think about it sir??
Dr. Bhavuk: I was.curious to know that weather a pre op sessions of RT will help in shrinking of tumor size, which will be followed by a wide local excision so ultimately leads to lesser post. Surgical morbidity Vasumathi Sriganesh, Bhavik Shah, Rakesh Biswas
Dr. Ishan: Sir I have read in some case reports and articles that this kind of tumor is radioresistant.. So I think surgery is the best treatment
Dr. Bhavuk: Can u please give reference, as I want to be.absolutely sure before I put my knife in.
Dr Ishan: Yes Sir.
Dr Rakesh: One of the other options discussed today with the radiation oncologist from Jawahar Cancer hospital, Bhopal by Dr Bhavuk is to utilize chemoembolization of the tumor feeder and then go ahead with surgery followed by radiotherapy. Dr Nitin would you be able to tell us who may be doing this in Bhopal? Dr Satish you have been trained in KEM for these above carotid interventions and it would be good to have your inputs.
Dr Rakesh: Dr Nitin and Dr Rahul, I was just looking at this report by you here of a similar patient in our journal IJUDH http://www.igi-global.com/article/case-study/124095 and interestingly Bhavuk, this patient had absolutely no bleeders.
Dr. Bhavuk: USG report says that the feeder vessels are pretty feeble, can we just go in and scope out the tumor, btw it has breached the cribriform plate, and is abutting the frontal lobe, so for sure a neurosurgeon is required, what opinion do all of u suggest, we recently spoke to radiation oncologist, he suggested us to undertake the patient for.chemoembolization for tumor to shrink and probably after a month take her up for surgery, but the patient is financially very vulnerable and cannot afford to go to another centre and get it done, I personally feel that at a given situation surgery is the only option ......
Dr. Vasumathi: After a one-to-one discussion with Dr Rakesh - am providing references to some large studies - I hope something turns out to be useful:
http://www.ncbi.nlm.nih.gov/pubmed/?term=Hemangiopericytoma[Mesh]+AND+systematic[sb]
The above was a link to reviews of literature
Here is a link to abstracts about radiotherapy or surgery
http://www.ncbi.nlm.nih.gov/pubmed/?term=Nose%5Bmesh%5D+AND+(Hemangiopericytoma%2Fradiotherapy%5Bmesh%5D+OR+Hemangiopericytoma%2Fsurgery%5Bmesh%5D)+AND+english%5Bla%5D+AND+hasabstract
Dr. Rakesh: Thanks Prof Upreet we saw and recorded it yesterday on a fundus photograph and it is normal. Wish we could upload the fundus images here which were taken by Hsiu An Lee.
Dr. Nitin: Could open only one image. From discussion, I presume that its primarily nasal growth with intracranial extension.
Combined craniofacial approach recommended for surgery. Pre-op embolisation good option. Surgery to be done within 48 hrs of embolisation.
Wide excision is not advised and vision can be saved. More detailed imaging would help to plan better.
Dr. Rakesh: Thanks Dr Nitin. I am tagging another of her CT images here:http://www.udhc.co.in/ViewImage?file_id=9499&scale=800. We also have her MRI (Dr Mridul) that is yet to be uploaded to her record (due to logistic reasons Kuldeep? Yogesh? Saurav?). We were unable to find anyone to do the chemo-embolization and have decided to go ahead with the caranio-facial approach led by Dr Bhavuk and Dr Mridul on Monday. Yogesh can you check if she has been put on the Monday OT list by Dr Bhavuk?
Dr. Yogesh: Sir, MRI report will be uploaded soon by Kuldeep. I am going to hospital and will let you know about the OT status.
Dr. Rakesh: Thanks Yogesh. Any luck with the MRI uploading so that Dr Mridul can plan accordingly?
Dr. Yogesh: It was closed due to Holiday.
Dr. Rakesh: Update: External carotid angiography and visualization of the tumor vasculature done yesterday by Dr Subroto and planned for pellet insertion to block both maxillary artery supply to the tumor today with pellet embolization followed by immediate OT with Dr Bhavuk, Dr Mridul, Dr Rahul (Inputs Dr Nitin) Dr Sadat, Dr Ashish, This patient was previously operated in 2012 in PCMS in the ENT department.
Dr. Rakesh: Dr Agamya's presence and help will be needed in the pellet embolization.
Dr. Sadat: As I correctly remember, this was a revision case of capillary haemangioma operated in PCMS. It was arising from ethmoids, was very vascular and we had to go step by step to remove the whole tumour endoscopically. Embolisation will definitely help.
Dr. Rakesh: Thanks Dr Sadat it appears to have transformed into an aggressive hemangiopericytoma (as in the recent biopsy) and here is the current tumor appearance of the patient: http://www.udhc.co.in/ViewImage?file_id=9476&scale=800
Dr. Sadat: Yes sir, I saw the reports.
Dr Rakesh: Unable to get the procedure done today due to a computer power out. Hope for tomorrow. :-)
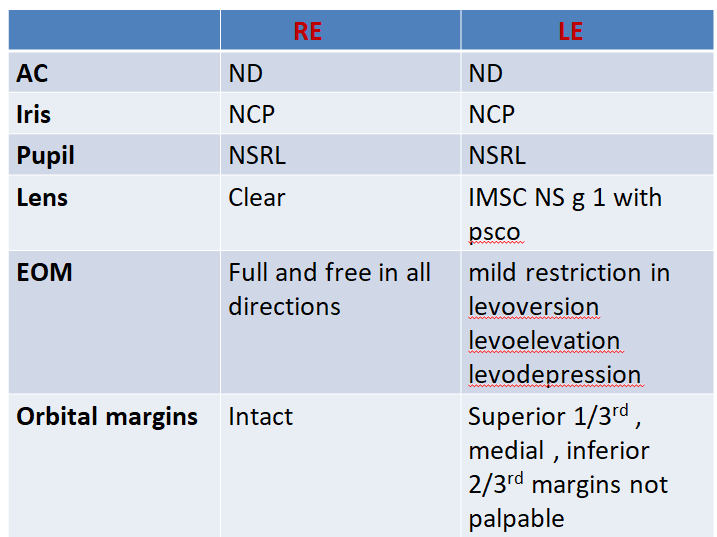
Dr Rakesh: Prof Upreet, Dr Satendra, Dr Rahul, Needed your inputs on an assumption put forward on 'why this patient has normal vision' by one of our colleagues. "We test vision with one eye closed. So while recording vision of the affected eye, as the other eye is closed the patient is managing to fixate with it may be by turning the eye or head. Thus recorded vision is normal?"
Thanks Prof Upreet, I did that today and found that she does have slightly reduced visual acuity in her left eye.
Dr Subroto, Bhavuk, Agamya, Hope we can nail her maxillary arteries tomorrow followed by OT either tomorrow or on Tuesday.
The patient was operated few days back after an embolization of her maxillary arteries by Dr Subroto and Dr Agamya

Dr. Rakesh: Other than the cosmetic appearance, her eye movement and vision is preserved. We are grateful to our surgeon Dr Bhavuk and his team (Dr Amit Jain, Dr Mriduli, Dr Pandya, Dr Saurav) and the medical students (Anuj, Utkarsh, Kashmoor) who donated their blood for this patient.

Dr Rakesh: DrIshan, Dr Vandana, I hope you have received the post op specimen.

Dr. Vasumathi: Wow. What a relief to see her face now! Hats off to the team
Waiting to hear more as investigations happen!
Dr Rakesh: Thanks Vasumathi for helping this patient with your literature search and thanks everyone for following her and supporting her.
Dr. Mridul: Kudos to Dr bhavuk and untiring assistance and support by Dr amit Jain and others and wonderful team of anaethetist lead by Dr sumit bhargav.
Dr. Kuldeep: I have to congratulate my team, they worked so well and come forward to help the patient.
Dr. Parth: Congratulations to whole team...with Dr. Biswas and Dr. Bhavuk
Dr. Swagata: Today stitches were out. wound healthy.Dr bhavuk and team of dr biswas congrats
Dr. Vadhumathi: Feel like singing Aaalll eees well :)
Dr Rakesh: Dr Saba and Dr Bhavuk this patient is returning next week for her follow up to benefit again from the LNMCH oral surgery team.
Dr Amy price: This is excellent very interested in the followup
Dr Rakesh: Here's the current CT images on follow up (Dr Bhavuk, Dr Saba, Dr Anil, Dr Suman) http://globaludhc07.blogspot.in/2016/01/a-40-years-old-woman-with-nasal-tumar.html
Dr. Bhavuk: She has to be taken up for contrast CT
Dr Rakesh: Prakhar i have discussed with Dr Bhavuk and Dr Agamya. There is a possibility that the soft tissue inside the nasal cavity that is currently visible on non-contrast CT could be herniated brain tissue. We agreed that this could be ruled out on a cranial MRI. Please send the patient for a cranial MRI today.
Dr. Bhavuk: Sir, I suppose since the case had a definitive diagnosis so we should call her with the diagnosis of heamangiopericytoma and considering the fact that tumor was in the same region, we should keep our fingers crossed for recurrence as well. Well hoping for the best waiting for MRI nada discussion with Dr. Agamya Saxena and Mridul Shahi sir
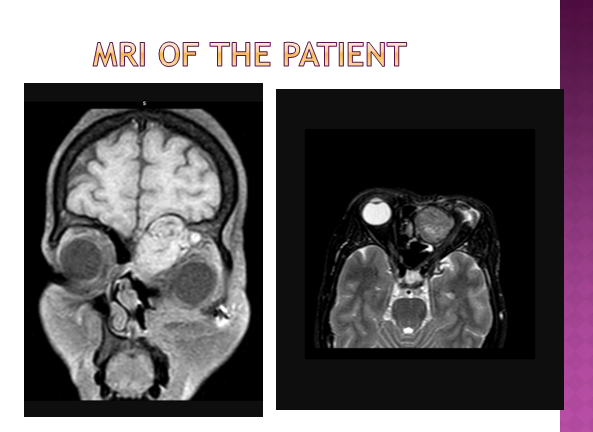
Dr. Rakesh: The MRI https://blogger.googleusercontent.com/img/b/R29vZ2xl/AVvXsEis-QZVuw5S_EpNaflYrNsIjDxYwnIgo3bfo0j4AE1DUPtoMOPBLSJPSuoOWKVlqKF1knTAENI2Jim1LsXvALPzaLKh4zkpQdxeNJrTn1yCSkvcoVMH_P7g4oA-4VMtFjAkkQzo_jllPLvN/s1600/she+401.jpg is very much suggestive of a recurrence. Looks like the end of the road for her? Any suggestions? (Amy, Kaustav, Bhavik, Prakhar)
Dr. Kuldeep: I think we want to find new way for her.
Dr. Nitin: Can we have more images? Did she receive radiotherapy post-op?
Dr Rakesh: Thanks Dr Nitin. There are many more images here:http://globaludhc07.blogspot.in/2016/01/a-40-years-old-woman-with-nasal-tumar.html She had another plastic surgery soon after to reduce the gaping in her initial wound and then had to go home 2000 kms away and this was one of the reasons post op RT was missed. What would be the possible option at this moment.
Can anyone add a physician from Jawahar cancer hospital, Idgah hills, Bhopal? (Dr Nitin, DrSaumya, Dr Preetesh). We need to ask them here (as the details are available here) if they can take her for RT now.
Dr. Nitin: Dr Gaurav Gupta, radiation oncologist
Dr Rakesh: Thanks Dr Nitin, can you add him here? It will become easier then to share the patient details with him for his further help
Dr Vinod, this is the patient Dr Varsha phoned you for.
Dr Mahawar, please share your thoughts here on this patient you saw today. regards, rb
Dr Gaurav will be good to have your inputs/queries on this patient. regards, rb
Mr Keshav please help us with arranging her radiotherapy through the CM fund (we also need to get her BPL card made).
Rajib and Tanmay for inputs on how to take this forward in Kolkata.
Sujoy it appears that the patient met Dr Lahiri in Chittaranjan cancer hospital, Kolkata but he wanted to see the images of his earlier CT, MRIs and histopathology slides that are accessible online from her record. Would it be possible for you to show these images to him? Rajib would it be possible for you to also help in collaboration with Sujoy?
Dr Sujoy: I have left CNCI 8 MONTHS AGO
Dr Rakesh: Thanks Sujoy, Yes but as you were in good terms with Dr Lahiri i was wondering if it would be possible to facilitate his viewing these images from here or perhaps even email. Our community health worker Mr Kar had asked for his email address but he said he wouldn't be able to access emails.
Dr Shaji, Dr Preeti this patient (see previous discussions as well as entire record above) has now received a suitable course of radiotherapy from Kolkata and has been currently advised to undergo surgery for removal of the residual tumor. She has already had 3 surgeries (one in North Bengal, one in PCMS, Dr Sadat Qureshi and one in LNMCH Dr Bhavuk Vanza).
Dr. Amy Price: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4179434/ Would Pazopanib after removing residual tumor be an option?
Dr Rakesh: Thanks Amy that would be too expensive for this patient.
Dr. Amy Price: very sad that life is income based
Dr. Rajib: is votrient is the same thing.. I think, it is available in the low-cost shop
west bengal govt is having few of these costly medicine available at a 75% reduced cost .. I can try to find out if I can get the exact name and dosage..
let me know if any governmental help and/or fund raising is required..
Dr. Rakesh: Avinash, Amy, Bhavik lets begin working on this patient. Her Community health worker is in touch with us.
Dr. Bhavik: I'm in! If we can get the signed consent form, that'd be great. I'll start writing soon!
Dr Rakesh:
Bhavik can we send her over to you at GCRI so that you can not only write about her but also help complete her treatment?
Dr. Bhavik: Yes, sure! That'd be great actually!
Dr. Rakesh: Have emailed her CHW to arrange that
Dr. Bhavik:
Alright! I'll meet the patient as soon as she reaches here.
Dr. Amy Price: Thanks Rajib and al look forward to writing too
Dr. Rakesh: Bhavik I guess you have met the patient there in GCRI now and we have run into the first stumbling block ( a perennial source of all our global health problems Rajib, Amy) and that is money. It appears they aren't able to afford the costs of the initial tests asked for in GCRI and are now wondering what to do after having made a 3 day train journey.
Dr. Bhavik: Yes, even I was not aware that GCRI (being a semi-government set-up) charges for initial hemograms. Since they have not carried the BPL card and also belonging the the other state, it is quite hard to get their treatment free. And the patient hasn't undergone a single scan/test since January 2016, so without the fresh reports, nobody would really see the patient. So, yes, it's a big problem indeed. I was equally helpless. And as far as I understand, the patient would end up being advised to take RT as she has already been operated three times. And the duration of RT is long. The patient seems unable to spend even a fortnight here. And their condition at large blocked my mind yesterday :(
Dr. Rajib:
where is the patient- is she is in bhopal.. this can't happen.. this is inhuman.. i will arrange for some fund.. let's at-least get her first test done... what will be the cost ..
... but I have to say this is the problem generally with the patient and patient relatives also from wb.. the perception is in govt hospital nothing will happen ..i somehow remember that they were supposed to come to kolkata and see a doctor in the govt setting - but i guess that never happened...or if they did they never informed me or gone to a pvt setting... i am screaming from the top - govt hospitals are doing great in west bengal..lots of problem true..but we have been able to get many people completelyy cured and treated in kolkata govt hospitals free of cost Papia Roy - one of our tireless volunteer can vouch for that.. we just had a 8 yrs old boy from kalimpong whose life was under danger is now in quite stable condition in NRS .. Rakesh - can you please convince them to come to kolkata to do the treatment.. instead of Chittaranjan, to me one of the medical college, such as RG Kar or PG can be a good place for treatment ..
Dr. Rakesh: Thanks Rajib, This patient did get treated in Chittaranjan cancer hospital for a while with radio therapy but the tumor recurred and they were bracing themselves up for another 4th operation in GCRI as Chittaranjan had apparently said that they may not be able to operate.
Dr Rajib: rakesh i don't think it makes sense for them to go through the OT in GCRI now.. it needs to be planned , get estimation from multiple places including govt hospitals in bengal if it's possible to do free, fund generated and then only they should travel..
Dr. Bhavik: GCRI is here in Ahmedabad. It's one of the best set-ups for cancer treatment in western India, probably next to Tata. Yet, it being a semi-government set-up, all the benefits are limited to the patients belonging to Gujarat. The cost of the surgery and/or RT would be nominal but the patients from other states have to pay for the initial investigations. And the same goes for this patient.
I am trying to help them as much as possible logistically, but the language barrier and the cost of living, unknown environment, rigid protocol at GCRI, etcetera would be too much for the patient :(
Dr. Rajib: don't mind Bhavik Shah - but this nominal can be too much for them.. it was at all not a good thing what they did.. without any planning just landed ..
can you get an idea of the cost ..approximate will do.. Rakesh - i believe you should convince them to come back..
Dr. Bhavik:Yes, I agree. Even I wasn't aware that they are costing 1500 for routine investigations and the same charges for CECT as other institutes. At civil hospital (my Alma Mater), everything is free. And CECT is done at 800. But as I mentioned already, GCRI being in the same campus, they're charging enormously.
I'm adding Shruti Gohel here to this group. She was my classmate and is R1 in RT there. We're figuring something out to help the patient somehow. If she's able to get her admitted, at least, they won't have to pay for the daily rent to stay here.
Dr. Rajib: yes do your best.. meanwhile Rakesh please talk with them..as i am sure they will listen to you . made them understand the situation.. it will be fool hardy if we exhaust our resources (whatever little it is) without getting the OT done or a long term treatment in place..
Dr. Rakesh:Thanks Bhavik and Rajib. My hunch is the folks at Chittaranjan cancer hospital, Kolkata ( a referral center for all cancer cases in West Bengal including IPGMER and RG Kar?) may have deemed a 4th surgery futile especially after the last extensive surgery that she underwent in Bhopal (Swagata) . However this patient is one girl who has the maximum amount of grit that I have ever seen. She would get herself operated a 100 times if she could find herself a surgeon willing to do it. Bhavik wish we had surgeons who had the time to not only operate but also pour over the tissue and find out solutions at a molecular level to prevent recurrence. This may become a reality Bhavik by the time you start operating?
Dr. Shruti: I can arrange for her accommodation here for as long as needed. I can talk to the Authority if we can arrange for the concessions in her treatment. Also, I can show the case to the senior Radiation Oncologists and take their opinion as to if we can directly take her for the Radiotherapy.
Dr. Rakesh: Excellent Shruti great to know you. Bhavik compared to her previous tumor extent recorded here : http://www.udhc.co.in/INPUT/displayIssueGraphically.jsp?topic_id=1780 what is the current extent of the tumor externally?
Dr. Shruti: Rakesh Biswas Sir : It's a pleasure and honour being a part of this endeavour.
Bhavik told me she has been advised a fresh CECT. But I think, if we have pre-op and post-op imaging available, we don't need her to undergo fresh imaging. We can simply get the previous imaging films reviewed at GCRI.
Dr. Bhavik: Her last MRI is from January 2016. So, I think anyone would like to have a recent scan. Plus, I don't think she has got the film of her last MRI as well :(
Dr Rakesh Biswas Thanks Shruti, They are all stored in multiple blog links above. Let me know if you are unable to find them. Also adding Ritu here who was my mbbs student at Manipal and later reviewed her before the 3rd surgery in Vydehi, Bangalore where she was doing her Mch (Boudhayan)
Thanks Bhavik, I think Kuldeep had sent her a CD of all her imaging done in Bhopal as that had been requested by the oncs in Chittaranjan
Dr. Bhavik: Oh alright! The patient is carrying a CD probably. Let's see, if Shruti can convince the consultants to get a review of the scan, it'll save this patient a lot of money.
Swagata Brahmachari :Yes Biswas Sir u are right.Her positivity is pulling her through.Still work at molecular level is way behind in India.
Rajib Sengupta great going guys. .. Bhavik and Shruti (nice to meet you virtually) ..i will bother you guys again - will it be possible for you guys to provide me a lump sum estimate (just approximate will do) for this operation, provided it cannot be done free ultimately (for whatever reason) Rakesh - no hunch please.. as you know things doesn't go so straightforward in WB hospitals specifically with many govt schemes going on (and changing everyday) .. can you please check with them (including talking with the physician from chittaranjan..the physician will talk with you , you being a physician) and get the exact story of what happened in Chittaranjan and what was the last treatment path that they suggested - sorry being a little stern - but I am sure you will not mind a little rebuke from your younger brother it's all for her benefit
Shruti Gohel: Rajib Sengupta Sir : Pleasure and honour meeting you . . . I will get the estimate by tomorrow. Tomorrow, Bhavik is going to bring the patient to GCRI. We'll sort everything together and keep posting the updates.
Kuldeep Gupta: okay sir i'll do. but where and how ?
Rakesh Biswas: Thanks Kuldeep you have already done it. Bhavik any updates?
Shruti Gohel: Patient was being consulted at the GCRI RT OPD today. She has been advised a fresh MRI as well as the histopathology slide review according to the institute protocol. She'll be reviewed after these investigations. We offered to admit her today. But they requested to get admitted tomorrow. Once admitted, their accommodation and meals will be free.
Rajib Sengupta: that's really great.. keep us updated Shruti.also I am assuming the treatment will be done free or minimal cost ?
Shruti Gohel: Meanwhile, I will re-sort all the relevant case-details from here. As the patient and the bystander understood only Bengali. I was lucky that one of my seniors is Bengali, so she helped me with history taking. Also, I am adding my Senior Consultant, Dr. Maitrik Mehta Sir to the group so that he too can go through the case details first hand.
Shruti Gohel: Rajib Sengupta Sir : I'll be able to give the estimate of the treatment only after the RT decision is taken. Shall keep updating.
Rajib Sengupta: great.. thanks a lot . Shruti for all the thing
Shruti Gohel Please don't thank me . . . It's an honour being a part of this noble endeavour . . .
Dr. Bhavik: Once I introduced the patient to Shruti, she has taken over from there very zeastfully. I'll keep track of the patient on a daily basis. Really grateful to her for helping this patient.
Dr. Rajib: I have added Dr Maitrik Mehta .. Welcome to our group Dr Mehta ..
Shruti Gohel: Latest MRI of the patient

Shruti Gohel: I will upload the films today once I get to the department of the Radio diagnosis.
She has been scheduled for the EUA and excisional biopsy for tomorrow
Dr. rakesh: Thanks a lot for these updates Shruti. Will be very keen to know the results of the excision biopsy too.
Dr. Shruti:






























































She has been scheduled for the EUA and excisional biopsy for tomorrow
Dr. rakesh: Thanks a lot for these updates Shruti. Will be very keen to know the results of the excision biopsy too.
Dr. Shruti:




Dr. Shruti: I will send pics today in better resolution as soon as I can. This is the procedure being advised. They have given estimate of ₹15,000 for this procedure. Patient is willing to undergo this
procedure.

Dr. rakesh: Thanks Shruti, the images suggest approximately similar growth size as in the previous recurrence? Heartening to see that she may get the procedure she needs. Wish this time we could do something better to prevent the next recurrence.
Dr. Shruti: Sir : Yes Sir
Dr. rakesh: Any updates, Shruti?
Dr. Suvra: Is it a recurrence? what was the previous biopsy diagnosis?
Dr. Shruti: Yes Sir!! Was just about to update on this. She got operated yesterday. Histopathology report awaited.

Rakesh Biswas: Excellent Shruti. Convey our regards to the operating team. Dr Swagata you had assisted in her last operation. Suvra yes this is her 3rd recurrence and 4th operation and the histopathology so far has been suggestive of Hemangiopericytoma.
Dr. rajib: so so thankful to Dr Shruti Gohel , Dr Maitrik Mehta and her team .. And obviously dr Bhavik Shah.
Rakesh Biswas, Boudhayan Dm, Abhijit Das - Can we have an estimate of such a procedure in a Kolkata Hospital?
Dr. bhavik: Thank you, but obviously, all the credit goes to Shruti. Since I am not a part of the institute at this very moment, my best bet was that Shruti would definitely take care of the patient, she being one of the very few compassionate doctors I know, around me, here at this place. The moment I agreed to have this patient come here for further management, I had that in mind actually. And, of course, she helped her way better than I could have. And, I would always be ready to help such patients in any possible way.
Shruti Gohel: Rakesh Biswas Sir & Rajib Sengupta Sir : Thank you for your kind words.  :) I was just doing my duty. Bhavik Shah !! Your support was no less!! :) A special thanks to Maitrik Mehta Sir for his support for the smooth proceedings. Here she goes!! All smiles!!
:) I was just doing my duty. Bhavik Shah !! Your support was no less!! :) A special thanks to Maitrik Mehta Sir for his support for the smooth proceedings. Here she goes!! All smiles!!

Dr. Shruti: Frozen section report.

Histopathology report is awaited.
Dr. rakesh: Thanks Shruti for sharing this image of an inspiring fighter. Vasumathi your inputs on her current image. Her left eye appears to be affected now?
Dr. rakesh: Shruti Gohel any updates?
Dr. Shruti: This is the Histopathological report of the Excision Surgery.


Patient had take Radiotherapy in August 2016. So, there is no role of Post-op RT at present.The patient went home after the suture removal. So, I collected the report on her behalf. She said, if needed, she'll come back.
Dr. rakesh: Thanks Shruti Gohel. The pathology team appears to have commented about their inability to access more clinical information on this patient.  😊 I wish we could have had them here. Suvra Biswas what is your opinion on the current biopsy findings? Swagata Brahmachari can we ask the previous pathology team for their comments on the current biopsy findings?
😊 I wish we could have had them here. Suvra Biswas what is your opinion on the current biopsy findings? Swagata Brahmachari can we ask the previous pathology team for their comments on the current biopsy findings?
Dr Shruti Gohel I hope you shall be able to write up this patient's story as a global health case report along with Bhavik Shah. Thanks for all your help for this patient.
They appear to have suggested immuno histochemistry. I wonder if they couldn't have done it on their own or were their issues of payment?
Dr. Bhavik: I believe that lab at GCRI is not that we'll equipped with IHC. Oftentimes, when needed, they outsource it. And I suppose IHC is pretty costly in private labs.
Dr. Suvra: current biopsy report is an insufficient description of the tumor. They should have written more elaborate description of the tumor for other features like vascular pattern ( staghorn ) and mitotic count. The biopsy images what you posted before ,although inadequate still I can see the features of Hemangiopericytoma which is a spindle cell tumor. It can have a differential with neural tumor from olfactory nerve - does she have any neural problem or any extension to cribriform plate? probably they want to do IHC to rule that out. But i go more in favour of Hemangiopericytoma with the clinical pic - female , nasal masss, high recurrence rate etc. But Mitotic count in the current biopsy slide ( which is not mentioned in the report)would help us to tell about the aggressiveness of the tumor.
Dr. Shruti: We have IHC facility available with GCRI. After primary Histopathological examination reporting, if IHC is advised, the relatives are given this option and if they want to go ahead with it, additional charges have to be paid. We could arrange for the free accomodation for the patient and her relative as well as free transportation to their hometown. But she had to bear the charges of the Surgery and the investigations. After surgery, she was in hurry to go home. Despite my persistent persuasion, she insisted on going home after suture removal. I asked them to wait till the HPE report of the Surgery comes. They said, they'll come back if needed but they absolutely wanted to go home then.
Suvra Biswas Sir : Sir!! If you'd like to see the images of the slides, I can try arranging them in 2-3 days.
Dr. Suvra: That will be great. I need some images with high magnification (>40x)
Dr. Swagata: Yes I will talk with Dr Vandana
UPDATES FROM HER HOSPITAL ADMISSION DURING THE WINTER OF 2018
Patient history before hospitalization:

Presentation notes containing the post hospital intervention part of her history:











Hand written notes containing the post hospital intervention part of her history:



Presentation notes regarding current situation of her nasal airway:



Presentation notes on her current vision status:





The current update and presentation notes on her facial restoration and support:



























Comments
Post a Comment