A Post-MI Asymptomatic Patient was Advised PCI and Stenting of Occluded artery: Is it really indicated?
A 55-year-old man developed sudden severe right sided chest pain at 1:00 AM. He thought the pain was related to gas and took acid reducing agents such as proton pump inhibitors but when the pain didn't get relieved by early morning he got admitted to a city hospital and the ECG (figure 1) was suggestive of an acute myocardial infarction. And a second ECG was done in the evening which showed qs pattern on the v1, v2, v3 and v4 (figure 2). His chest radiograph was done (figure 3). His past history was significant for a type II diabetes mellitus (on medication) for last 6 years and hypertension (on medication) for last 10 years.
 | |
| Figure 1 |
 | ||||||||||||
| Figure 2 |
 |
| Figure 3 |
He was not thrombolyzed but a coronary angiography was planned and was done eventually on the same day around 8 P.M. The coronary angiography revealed (figure 4, 5, 6, 7, 8, 9, 10) 30% plaque in proximal & mid part of LM, 95% stenosis in LAD and minor irregularity in LCX distal part and he was advised stenting but the patient was unable to afford the cost. He came to our hospital a few days later and following a clinical cardiology evaluation he was insisted on another coronary angiography and advised stenting and when the patient was asymptomatic. No other options were discussed although medical management including antiplatelets and statins were continued.
 | |
| Figure 4 |
Figure 8
Figure 9
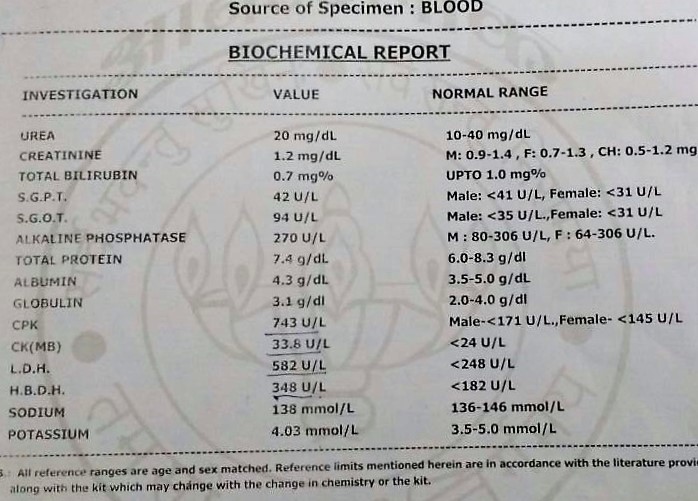
Other investigation results are as follows:






Now the question arises:
1. Is it really indicated to give reperfusion therapy/PCI in these asymptomatic patients days after the initial myocardial infarction to open up the occluded arteries?
2. If not then why are these interventions needlessly done for many patients globally?
3. What would be the best way to address this issue?
Conversation around this case:
Rakesh Biswas Aadipta Ghosh, Indranil Dev, for your inputs with regard to Vivek Poddar'S query.

Indranil Dev If the patient is absolutely asymptomatic with an occluded artery and 48 hours have passed from onset of pain PCI is not indicated
Indranil Dev If heart failure is present and critical disease in a proximal infarct related artery is present - stabilise with diuretics, then look for hibernating myocardium ( dobutamine stress echo or a thallium) - if large viable area consider PTCA

Rakesh Biswas Thanks Dr Indranil. Vivek can we share the echo and 1st coronary angiography report of the patient here. Dr Indranil given that the patient is asymptomatic and given the last angiography (done on day one of myocardial infarction) and echo report would you need to intervene with another angiography if the patient presented within a week of the first angiography?



Vivek Poddar Angiography videos can be found here http://bmjcaselogvivek.blogspot.com/.../a-post-mi...



Ambarish Bhattacharya All international guidelines advocate primary PCI. There's actually a door-to-needle time too.
The question to be answered here is why was PCI delayed?
The question to be answered here is why was PCI delayed?
Rakesh Biswas Good question Ambarish. Vivek please share some more history here to explain the delay
Vivek Poddar Ambarish Sir, the patient had the initial symptom began around 1 am and since then patient was thinking it of indigestion and was trying to take acid reducing agents. But when it didn't get relieved, patient was taken to the hospital on the same day ar...See More
Ambarish Bhattacharya Whatever delay patient has done is beyond your control.
Don't delay what is within your powers
Don't delay what is within your powers
Vivek Poddar Yes sir. How could we solve and address the issues that patients presenting after few days post-MI and PTCA and stentings are still indicated. What are the attempts we can make to solve this needlessly done interventions where poor patients cannot even afford it, as in this case patient refused to undergo the intervention.

Bhavik Shah We should keep in mind here that 'door-to-needle' time, 'door-to-balloon' time, and 'PCI related delay' are useful in determining the efficiency of the centre. Normally, door-to-needle time should be less than 30-45 minutes and door-to-balloon time should be 90-120 minutes.
Now, PCI should be considered over thrombolysis in quite many instances but the main points include:
1) The patient has significant bleeding risks
2) The patient is in grave condition, i.e., cardiogenic shock
3) Diagnostic dilemma
Considering the condition of this patient,
"Registry data suggest that 9 to 31 percent of patients with STEMI present more than 12 hours after the onset of symptoms. Primary PCI may be of benefit in some patients, particularly if symptoms of myocardial ischemia are present. In asymptomatic, stable patients who present after 12 hours, there is no evidence that reperfusion with either fibrinolytic therapy or primary PCI is of benefit."
References for the quote above:
https://www.ncbi.nlm.nih.gov/pubmed?term=14532318
https://www.ncbi.nlm.nih.gov/pubmed?term=11844506
Now, PCI should be considered over thrombolysis in quite many instances but the main points include:
1) The patient has significant bleeding risks
2) The patient is in grave condition, i.e., cardiogenic shock
3) Diagnostic dilemma
Considering the condition of this patient,
"Registry data suggest that 9 to 31 percent of patients with STEMI present more than 12 hours after the onset of symptoms. Primary PCI may be of benefit in some patients, particularly if symptoms of myocardial ischemia are present. In asymptomatic, stable patients who present after 12 hours, there is no evidence that reperfusion with either fibrinolytic therapy or primary PCI is of benefit."
References for the quote above:
https://www.ncbi.nlm.nih.gov/pubmed?term=14532318
https://www.ncbi.nlm.nih.gov/pubmed?term=11844506
Ambarish Bhattacharya Exactly
Rakesh Biswas Sivapuram please upload the echo report of this patient here. Moynul , Vivek please share the video link of his echo here. We need to know from Dr Indranil after he goes through the echo if we can get a TMT now to assess his effort tolerance
Rakesh Biswas Also Sivapuram please share his coronary angiography video link here







Vivek Poddar Angiogram videos are uploaded on the blog link posted above.
Manage
Rakesh Biswas Thanks Vivek and the echo and angiography written report


Rakesh Biswas Dr Indranil going by the coronary angiography report above in this patient who became asymptomatic in a week after his myocardial infarction would it have been useful for the patient to have gotten a stent as advised in the coronary angiography report?
Indranil Dev No. If there is no post mi angina it would signify that viable myocardium is likely to be present. If echo shows thinned out myocardium in the affected territory then Ptca would no longer be indicated. Here it's only akinetic so another test like dobutamine stress echo may be indicated.
Indranil Dev Sorry viable myocardium is unlikely to be present- correction.
Comments
Post a Comment